(新)眼皮 割雙眼皮 眼皮整形 縫雙眼皮 雙眼皮手術 公告:請先矯正屈光不正.再進行雙眼皮手術.萬分感激.
公告:請先 矯正屈光不正 .再進行雙眼皮手術.萬分感激.
anatomy-physiology-of-eyelids-15-638.jpg
「 眉目傳情」,這是描寫美麗動人心靈之窗的眼睛,所表現出的的各種情感活動。然而什麼樣的眼睛才算美呢?或許有人會說一雙炯炯有神的大眼睛,雙眼皮再配上墨黑的雙眉這就是美。
其實,這還不足夠,尚須與面部其他器官(如臉形、鼻形、內外眼角間距、嘴形)協調一致,才較為理想。
雙眼皮類型
封閉式(內雙) 半開放式 (東方)) 全開放式 (西方)
雙眼皮種類105-09-05. - 複製.jpgeyelid classification - 複製.jpgcgm9564e7a92b2ffb17201b12592add2c45482.jpg
雙眼皮手術成功的標準
雙眼皮的手術成功,因為個人的審美觀點不同,很難一致認定。
但雙眼皮看起來自然、對稱則是成功的基本標準。術後雖有刀痕,但因隱藏在雙眼皮皺摺內,故睜眼時是看不到的。
不宜做雙眼皮
.兩眼間距離近的人,手術後效果較不理想。
.圓形眼的人此時需合併其他手術(隆鼻術、內眥贅皮整形)來改善。
.有嚴重內科疾病。
.眼睛患眼疾時,暫不宜做雙眼皮手術。
手術方式 : 依年紀及眼皮鬆弛程度,可分為下列:
雙眼皮縫合手術(縫合式雙眼皮手術) 雙眼皮切割手術 (切開式雙眼皮手術)
原理 兩眼各 5 針皮下埋線方式。 切除 上眼皮多餘的脂肪 同時可將多餘的眼皮脂肪做切除 。
優點 手術時間短、傷口小、恢復期短、消腫快、術後不必拆線、手術 滿 3 天後就不太會腫。 持久的眼皮手術 。
缺點 雙眼皮鬆開的機會比較高,看縫合技巧而定,也可維持永久。 2-3 年後約有 2 成的人會因縫線被吸收而恢復原狀。 切開的皮膚會留下疤痕且浮腫期較長。 手術後 1 個月,看起來比較自然。
適用對象 眼皮較薄、皮下脂肪少、眉眼間距較短者。 眼睛較浮腫、眼皮較厚、眼皮下垂、眼皮脂肪過多、睫毛倒插、上眼皮的皮膚鬆弛或過多,去除不需要的皮膚或脂肪。
手術時間 約 40 分 約 1.5 小時
麻 醉 局部麻醉 局部麻醉
復原時間 約 5-7 天,愈年輕復原速度愈快 1 週消腫,但 約 1-2 月才會
術後照顧
42小時內冰敷數次(1次15-30 分鐘),3天後改溫敷,以利退瘀消腫。
• 以無菌棉棒沾生理食鹽水清潔,塗抹消炎藥膏避免感染。
• 避免菸、酒、辣椒、等刺激性食物。
• 避免長時間視線往下閱讀或打電腦。
• 不需拆線。
請依照醫護人員指示回診,並按時服藥、冰敷、避免搬重物、低頭及俯臥趴睡等 。
術後照顧同左。
• 1 週後拆線,拆線後回家可洗臉碰水,但不可用力去揉。局部可擦上抗疤凝膠,或眼尾會貼上膚色透氣紙膠至少二個月,進行疤痕護理。
請詳閱完上列內容以及內文之超連結,謝謝。
下列為諮詢影片,僅供參考。
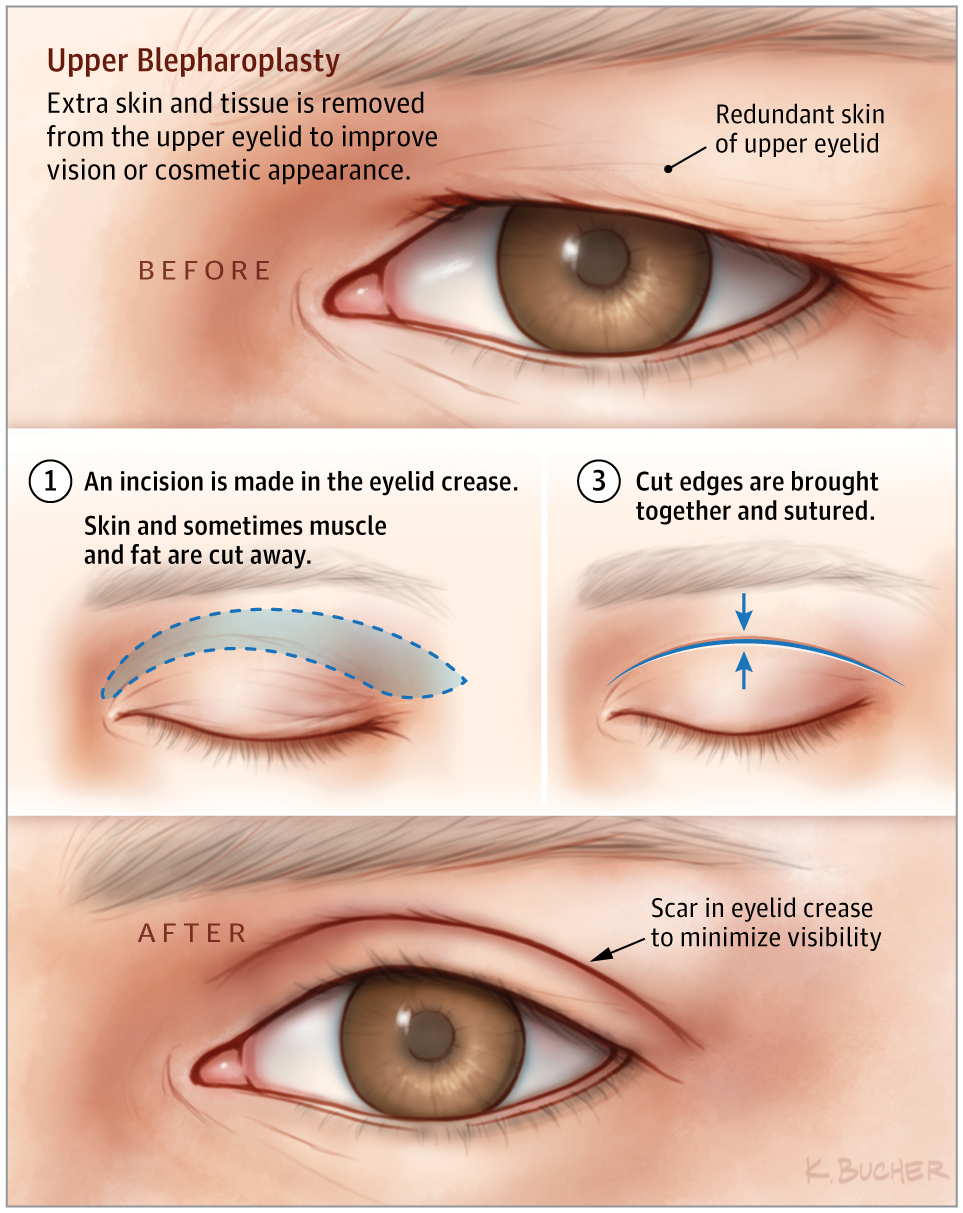
Upper blepharoplasty is a procedure that involves resection of redundant skin and/or musculature of the upper eyelid.
Aging of the Upper Eyelid/Brow Complex
With aging, a patient may notice the upper lids feel “heavy.” This can be caused by the eyebrow descending, upper eyelid skin excess, or both. Upper blepharoplasty, or eyelid lift, is distinct from a brow lift, which elevates the eyebrow. These procedures may sometimes be done together.
Reasons for undergoing an upper blepharoplasty may be purely cosmetic (to reduce the appearance of aging), functional (to reduce obstruction of vision by overhanging skin), or both. Functional upper blepharoplasty involves reduction of the upper eyelid to improve visual obstruction caused by redundant lid tissue. Patients may seek cosmetic upper blepharoplasty with aesthetic concerns regarding overhanging skin, which may cause a less youthful appearance. Clinical evaluation and management of both functional and cosmetic concerns is important. In addition, any ptosis of the upper eyelid (meaning that the margin of the eyelid sits too low and covers the pupil) should be noted. This is caused by poor function of the muscles of the eyelid and is treated differently (ptosis repair).
Patients with eye disease such as glaucoma or dry eye are not candidates for eyelid surgery except in special circumstances.
Basics of Upper Blepharoplasty
The procedure may be done with local or general anesthesia. Technically, the procedure involves identifying the upper eyelid crease on each eyelid and designing a skin excision that removes enough skin to alleviate the issue and preserves enough to allow normal eyelid closure. In some cases, a small amount of the orbicularis oculi (the muscle that closes the eyelid) is removed. Fat is typically preserved over the middle of the eyelid, but some removal may help with aesthetic contour in cosmetic eyelid surgery. When the procedure is complete, the eyelid is closed with sutures. The incision should lie in the eyelid crease, making it less visible after healing.
Recovery
Typically, patients may have mild bruising or swelling around the eyes for 10 to 14 days. Some surgeons may recommend avoidance of makeup for 2 to 3 weeks. Glasses may be worn immediately, but patients may be instructed to avoid contact lenses for a few weeks, depending on surgeons’ preferences.
Complications of blepharoplasty are relatively rare. The primary issue to consider is removal of too much upper eyelid skin, resulting in difficulty closing the eye. This in turn may cause chronic dry eye issues and pose a risk of injury to the cornea. For this reason, conservative skin excision is recommended. Other complications include ptosis of the eyelid (due to injury of the levator muscles), asymmetry of the eyelids, or blindness, which is exceedingly rare.
For More Information
- American Society of Plastic Surgeons
www.plasticsurgery.org/cosmetic-procedures/eyelid-surgery
To find this and other JAMA Patient Pages, go to the For Patients collection at jamanetworkpatientpages.com.
The JAMA Patient Page is a public service of JAMA. The information and recommendations appearing on this page are appropriate in most instances, but they are not a substitute for medical diagnosis. For specific information concerning your personal medical condition, JAMA suggests that you consult your physician. This page may be photocopied noncommercially by physicians and other health care professionals to share with patients. To purchase bulk reprints, call 312/464-0776.
Back to top
Article Information
Conflict of Interest Disclosures: None reported.
Source: Weissman JD, Most SP. Upper lid blepharoplasty. Facial Plast Surg. 2013;29(1):16-21. doi:10.1055/s-0033-1333833





